
Pain Management
Understanding your options and what feels right for you
Every labour is different. Understanding your options for pain relief can help you feel more confident, in control, and supported during your birth.
Understanding Your Options
As you get ready to welcome your baby, you may not have spent much time thinking about pain relief – and that’s completely understandable. Still, taking a little time now to explore your options can make a real difference.
By learning about the medicines, techniques and alternatives available, you can feel more confident, more in control, and well supported when your big day arrives.
Pain Relief in Labour
You may already be familiar with epidurals, but there are several other pain relief options available to you as well. Taking the time to explore these can help you choose what feels right for your body, your birth, and your preferences.
Depending on your individual circumstances, you might consider:
Gas and air (Entonox)
This is a mixture of 50% oxygen and 50% nitrous oxide, inhaled through a mouthpiece to provide short-acting pain relief. Because you administer it yourself, many women appreciate the sense of control it offers. However, some experience side effects such as dizziness or nausea.
Using the hydrotherapy pool
At the National Maternity Hospital, you may have the option to labour and give birth in a warm water birthing pool*. Being immersed in warm water can help to ease contraction pain and promote relaxation for some women.
Transcutaneous Electrical Nerve Stimulation (TENS) machine
With this method, small pads are placed on your back and connected to a handheld device that delivers gentle electrical impulses through the skin. TENS can be particularly helpful in early labour. Please note that you’ll need to bring your own TENS machine, as these are not provided by the hospital.
Remifentanil
This is a strong, short-acting pain relief medication given through a drip*. You control when you receive a dose by pressing a button, allowing you to manage your pain as needed. Remifentanil cannot be used at the same time as an epidural. While it can be effective for contraction pain, it would not provide enough pain relief for a Caesarean section. Remifentanil patient-controlled analgesia (PCA) is available at the National Maternity Hospital.
*Not yet available at all maternity hospitals.
The Truth about Epidurals
Epidural analgesia is the most effective and reliable form of pain relief available during labour, and it has a very strong safety profile. You may have come across mixed messages online or on social media, or in older books – and these don’t always give the full picture.
At The National Maternity Hospital, epidurals are a common and well-established option. In 2024, 61.7% of women who had a vaginal birth chose to have an epidural. Of those, 81.4% were first-time mothers, while 59.7% were having their second or subsequent baby.
Myth 1: “Epidurals cause chronic back pain”
False.
You might hear that back discomfort after labour is linked to having an epidural. While some women do experience back pain, there’s no evidence that epidurals are the cause (1). Pregnancy itself – along with any pre-existing back problems – is much more likely to be the reason.
Myth 2: “An epidural will slow my labour down”
Partially true.
Epidurals can make labour a little longer, but the difference is usually quite small. On average, they extend labour by around 15 minutes over its full duration – a change that many women feel is manageable in the context of effective pain relief.
Myth 3: “If I get an epidural I’ll end up needing a Caesarean section”
False.
Epidurals do not increase your risk of needing a Caesarean section – something that has been shown in several large studies. Research also suggests that epidurals can make labour safer (2), especially if you have certain medical conditions (3).
Myth 4: “There’s only a small window of time to get an epidural”
False.
While it’s best not to leave it until the very last moment, you can usually ask for an epidural at any stage of your labour – as long as there’s enough time for it to take effect. If your labour is moving quickly, for example in a second or subsequent birth, your baby may arrive before the epidural has time to work.
Your care team will always be there to guide and support you. Because maternity care can sometimes involve urgent situations, there may be occasions where your anaesthesiologist is needed elsewhere in an emergency, which could mean a delay in placing your epidural.
You can feel reassured that your midwife will help you make decisions about the timing – they have extensive experience supporting women through these choices. At The National Maternity Hospital, families consistently tell us how supported and empowered they feel, thanks to the care and expertise of our midwifery team.
Myth 5: “Epidurals can cause nerve damage”
Partially true.
While this is possible, it is extremely rare. If nerve damage does occur, it’s much more likely to be related to the birth itself – for example, from prolonged pushing or pressure on the nerves inside the pelvis from your baby.
To help reduce this risk, your midwife will encourage you to change your position regularly during labour. At the National Maternity Hospital, we also use a ‘regional anaesthesia alert bracelet’ to support you in getting moving again as soon as you feel ready after your baby is born, as early mobilisation can help minimise symptoms of nerve damage.
Myth 6: “The drugs in the epidural might harm my baby”
False.
The medications used for epidurals are safe for both you and your baby during labour, and they do not interfere with breastfeeding.
At the National Maternity Hospital, we are always reviewing and refining our care – regularly auditing our practice and listening to feedback from women – to ensure we use the lowest effective doses of medication while still providing excellent pain relief.
References
(1) Timerga, Sara, Walle, Getaw, Mebratu, Wondwosen, Befkadu, Aynalem, Assessment of the Association Between Neuraxial Anesthesia and Back Pain After Delivery: A Systematic Review and Meta-Analysis, Anesthesiology Research and Practice, 2025, 2105413, 16 pages, 2025. https://doi.org/10.1155/anrp/2105413
(2) American College of Obstetricians and Gynecologists Committee on Obstetric Practice. ACOG committee opinion. No. 339: Analgesia and cesarean delivery rates. Obstet Gynecol. 2006 Jun;107(6):1487-8. doi: 10.1097/00006250-200606000-00060. PMID: 16738188.
(3) Kearns RJ, Kyzayeva A, Halliday LOE, Lawlor DA, Shaw M, Nelson SM. Epidural analgesia during labour and severe maternal morbidity: population based study. BMJ. 2024 May 22;385:e077190. doi: 10.1136/bmj-2023-077190. PMID: 38777357; PMCID: PMC11109902.
Caesarean Section
Many women plan for a vaginal birth, but sometimes your baby has other plans – and a caesarean section is needed. In Ireland, 41.5% of first-time mothers give birth this way.
At The National Maternity Hospital, we focus on making your experience as personal and comfortable as possible. Our award-winning ‘Sips Til Section’ initiative allows you to drink water freely before your operation, and you can listen to your own music in theatre using an iPad and speaker*. You’ll also be encouraged to eat and drink as soon as you feel ready afterwards.
Your anaesthesiologist will stay with you throughout the procedure and will see you again the next day. You’ll also meet an anaesthesiologist at your antenatal classes to help you understand what to expect and answer any questions.
After your caesarean, you may be offered paracetamol. Taking paracetamol and ibuprofen regularly can reduce the need for stronger opioid pain relief, in line with international best practice to support your recovery.
Want to learn more?
Here are two excellent resources to guide you:
- www.labourpains.org – created by anaesthesiologists, with clear and honest information
- www.nmh.ie – the National Maternity Hospital website, where you’ll find detailed information on your options under Maternity → Labour and Birth → Pain Management
Remember, if your birth doesn’t go exactly as planned, you’ve done nothing wrong – not everything can be predicted or controlled. Every birth is unique. Your anaesthesiologist is a specially trained doctor, and many of us are parents too – we all want the very best for you.
What you can do is come informed and prepared – and we’re here to support you every step of the way.
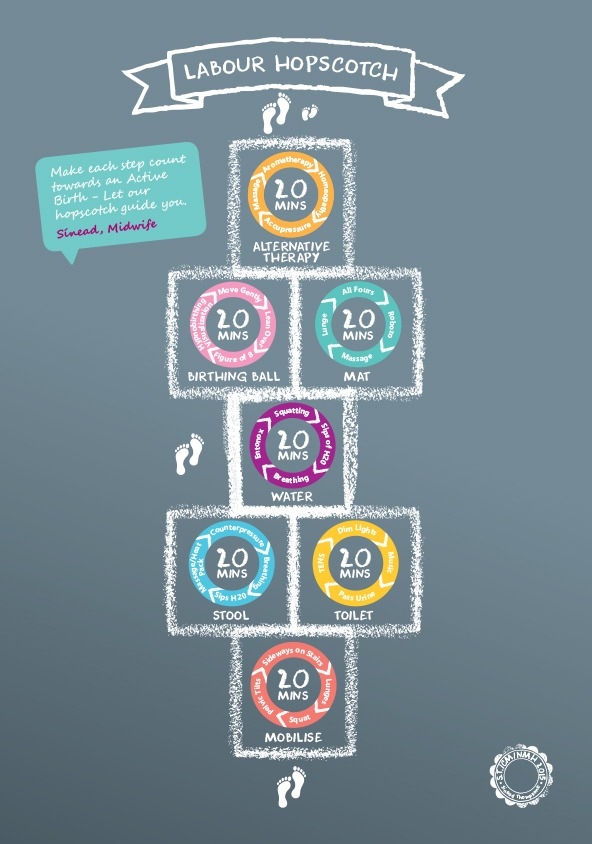
Labour Hopscotch Framework
Welcome to the Labour Hopscotch framework, developed by Sinéad Thompson, community midwife at the National Maternity Hospital. This simple tool is designed to support you through your labour journey.
You can begin using it at home – starting at the bottom of the hopscotch and moving through each step as labour progresses. Each stage is illustrated in sequence with guidance on timing, helping you feel focused and reassured along the way.
As you move forward, you’ll reach baby’s footprints – a motivating image to help you visualise your progress and stay centred. We hope you find it a helpful and encouraging guide.
{kind=link}
Summary of Pain Management Options
Labour Hopscotch – make each step count
A visual tool to support an active birth, guiding you through 20-minute rotating steps during labour – such as walking sideways on the stairs or sitting on a stool with massage – to help keep you moving, focused and comfortable.
TENS (Transcutaneous Electrical Nerve Stimulation)
A handheld device delivering gentle electrical pulses through pads on your back. You control it yourself, helping with movement, distraction and comfort, while also encouraging the release of your body’s natural pain relief – endorphins.
Hydrotherapy Pool
At The NMH, 12 birthing rooms support the use of water, either in a pool or shower. Warm water can create a calm environment, ease movement and improve comfort. See our Birthing Pool for Labour and Birth Information Booklet.
Entonox (gas and air)
A mix of nitrous oxide and oxygen, inhaled through a mouthpiece during contractions. It supports slow, deep breathing and allows you to stay upright and mobile. Some women may feel drowsy or nauseous.
Pethidine
A morphine-related injection that acts as a sedative and muscle relaxant. It can reduce pain and tension, often allowing you to rest between contractions. Nausea is common, so an anti-sickness medication is given alongside it.
Epidural Analgesia (labour)
Given by an anaesthesiologist into your lower back, this provides very effective pain relief, leaving you numb from your upper abdomen down. You’ll need a drip in your arm, continuous monitoring of your baby, and regular bladder care with a catheter. You’ll remain in bed during labour and for about 6 hours after birth.
Please read the Information Card on Epidural Analgesia for Labour Pain for important details and risks.
Epidural/Spinal Anaesthesia (caesarean section)
Most caesarean births are carried out using spinal or epidural anaesthesia, so you’ll be awake to meet your baby. You’ll be numb from your upper abdomen down and unable to move your legs for up to 3 hours, with walking usually possible again after about 6 hours. In urgent situations, a general anaesthetic may be required.
Please read the Information Card on Epidural/Spinal Anaesthesia for Caesarean Section for important details and risks.
For general information on pain relief choices during labour, please see labourpains.org
For further information please visit our Labour and Birthing Unit page.